

From preclinical studies to first-in-human trials, GMP-compliant 3D printing platforms deliver automated capsule filling at up to 10,000 units per day per unit, bringing precision and cost-efficiency to the volumes that matter most in early development.
The small-batch problem in pharmaceutical manufacturing has never solved
Drug manufacturing has always operated between two extremes. At one end sits the high-throughput commercial manufacturing plant, engineered and validated to produce millions of units annually with tightly controlled processes. At the other stands the compounding pharmacist or formulation scientist preparing doses by hand, weighing powders and filling capsule shells one tray at a time while hoping that batch-to-batch variability stays within acceptable limits. Between these two poles lies a persistent, underserved gap: the need for batch sizes up to a few thousand units, produced with the rigour of the mass-production quality standards but at much smaller scales and physical footprint.
This is the reality facing pharmaceutical companies when reaching the stages of conducting preclinical toxicology assessments, first-in-human (FIH) trials, and Phase I dose-escalation studies. Quality requirements are too stringent for manual compounding, but the required volumes are too small to justify a full manufacturing run, and even scaled-down process equipment lacks the desired production flexibility. The resulting solutions have often been straining timelines and budgets through the reconfiguration of processes or extensive waste of supply. For hospital and community pharmacies, the challenge is slightly different but equally acute. Every day, pharmacists prepare individualised doses for patients with non-standard requirements (i.e. paediatric populations, patients with renal or hepatic impairment, or those requiring combinations not available commercially) using processes that remain largely manual, time-intensive, and prone to variability.
It is this gap between compounding and large-scale industrial production that a new generation of GMP-certified pharmaceutical 3D printers is now targeting. These low-footprint platforms are designed specifically for automated capsule and blister filling at the volumes that matter in early pharmaceutical development and in compounding pharmacies. With a throughput of up to 10,000 dose units per day from a single, compact instrument, the 3D printers are rapidly becoming an established platform for pharmaceutical companies, contract research organisations (CROs), clinical trial supply teams looking to maximise their development workflows, and compounding pharmacies.
A maturing technology landscape
Pharmaceutical 3D printing is no longer a research curiosity. The sector has progressed from academic proof-of-concept to commercially deployed GMP systems operating in clinical and pharmacy settings around the world. The landmark that framed its regulatory credibility was the FDA approval of Aprecia Pharmaceuticals’ Spritam (levetiracetam) in 2015, the first 3D printed drug product to receive regulatory clearance. Made using Aprecia’s proprietary binder-jetting ZipDose technology, Spritam demonstrated that additive manufacturing (3D printing) could produce dosage forms meeting commercial pharmaceutical standards, establishing a regulatory precedent that the rest of the sector has built upon. Since then, pharmaceutical 3D printing has evolved along several technological and commercial pathways. The major printing modalities in active GMP deployment today include semi-solid extrusion (SSE), melt extrusion deposition, and binder jetting, each with distinct formulation requirements, processing characteristics, and output capabilities.
Semi-solid extrusion: the science that makes it work
While several pharmaceutical 3D printing technologies exist, the technological foundation of the 3D printing capsule- and blister filling platforms is the semi-solid extrusion (SSE) modality. SSE operates at ambient or gently elevated temperatures, minimising the risk of compromising active pharmaceutical ingredient (API) physical integrity because of high temperatures.
In practice, the process begins with a pharma-ink, which is the developed SSE formulation in which the API is either dissolved or uniformly suspended in a matrix carrier with shear - or temperature-dependent semi-solid properties. Excipients are selected to provide adequate rheological characteristics and are selected based on chemical compatibility and stability. The pharma-ink is loaded into sterile precision syringes, followed by extrusion through nozzles of interchanging dimensions under steady pressure to deposit exact quantities directly into capsule shells or blister packages. Dose manipulations are easily enabled in the steady flow-state of pharma-ink by the linear relationship with the magnitude of extrusion force. The output is a dosage unit in which dose uniformity is a function of engineered process control, and it can take the form of a 3D printed, layered tablet, a filled capsule, or filled blister packages.
The scientific case for SSE in pharmaceutical production is supported by a growing body of peer-reviewed evidence. Published in a leading pharmaceutical sciences journal, Pfizer demonstrated that SSE 3D printing can successfully maintain crystalline solid dispersions, a critical consideration governing bioavailability and in vivo performance. The study developed pharma-inks incorporating both high-solubility and low-solubility drugs at levels ranging from 0.2% to 30% w/w and successfully printed dose-flexible tablets suitable for both preclinical and FIH use. Crucially, the gentle processing conditions preserved each API's polymorphic form throughout.
This combination of formulation and process flexibility, mild processing conditions, and precise volumetric control makes SSE uniquely suited to the demands of early pharmaceutical development, where the API supply is limited, the formulation is still evolving, and the analytical burden of demonstrating dose uniformity must be met at every stage.
Platforms built for GMP environments
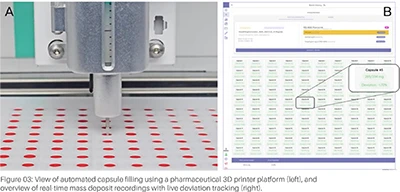
There is an important distinction between a 3D printer adapted for pharmaceutical use and one designed and built for the purpose of being used in GMP-regulated pharmaceutical environments. At the heart of the platforms’ quality assurance capabilities are integrated analytical balances that provides 100% gravimetric verification in real time. Every capsule or blister cavity filled during a production run is individually weighed, with fill weights automatically captured and compared against pre-specified tolerances. Any unit falling outside the acceptance criteria is immediately flagged, and the data are captured in a complete electronic batch record. This level of in-process weight verification ensures compliance with uniformity of mass requirements; all performed in an automated fashion.

Complementing gravimetric control, the pressure sensor monitors pharma-ink flow continuously throughout the extrusion process. Anomalies indicating a clogged nozzle, entrapped air, or a shift in ink viscosity are detected in real time, enabling immediate intervention before out-of-specification units are produced. This closed-loop process monitoring is central to the platforms’ GMP credentials where deviations are caught and addressed during production, not discovered retrospectively during quality review. With the additional near-infrared spectroscopy sensor and software components, data pertaining to drug quantities can be verified in the individual dose units, offering further quality checks.
The software integrates all the applicable functions and maintains comprehensive, audit-trail-enabled electronic batch records, capturing operator actions, process parameters, fill weights, deviations, and timestamps in a format consistent with 21 CFR Part 11 and equivalent regulatory expectations. Excipient and protocol libraries enable easy access and overview of multiple projects. This documentation capability is not merely a convenience; it is an enabler for regulatory submissions.
From a throughput perspective, up to 10,000 capsules can be manufactured per day from a single 3D printing unit. For development programmes or clinical trial supply operations requiring greater daily capacity, multiple platforms can operate in parallel to scale production linearly.
Accelerating preclinical and clinical development programmes
The value proposition of flexible, small-scale manufacturing platforms in early pharmaceutical development is clearest when considered against the specific demands of preclinical and clinical workflows.
In preclinical work, dose flexibility is paramount. Animals are typically dosed across a range of body weights and study designs, requiring multiple dose strengths from the same formulation. With traditional manufacturing approaches, each dose strength requires a separate batch, with all the associated resource and timeline implications. The 3D printing workflow eliminates this constraint, where a single pharma-ink can be used to produce any required dose simply by adjusting the programmed fill weight. Multiple strengths can be generated in a single production session from one validated ink. This flexibility not only accelerates study setup but also ensures formulation consistency across dose groups, key for pharmacokinetic interpretation.
For FIH and Phase I clinical trials, the precision of the filling process and the integrity of the batch record are directly relevant to regulatory submissions. Dose escalation designs, which may require the production of four, six, or more different strengths in small quantities, are managed with equal ease, using the same pharma-ink and the same automated platform. The 100% weight verification and automated documentation provide the quality evidence that underpins regulatory requirements.
The clinical utility of the pharmaceutical 3D printers has been demonstrated through their deployment at Gustave Roussy Cancer Campus, Europe's leading oncology research institution. While it is now routinely used as a highly flexible compounding platform, its capsule filling technology was proven more than capable of supporting in-house production of five different targeted combination interventions for a six-month clinical trial in 200 breast cancer patients.
Expanding into community and hospital pharmacies
While the GMP certifications make the platforms a natural fit for pharmaceutical companies and CRO environments, the same precision and automation advantages translate directly to compounding settings, whether in community or hospital pharmacies, to improve current workflows. Compounding pharmacies preparing extemporaneous formulations for patients with non-standard dosing requirements would benefit from automated production of high-quality small batches.
A study conducted at a compounding pharmacy in Madrid evaluated a 3D printing platform for routine minoxidil capsule production for nine patients receiving personalised doses. The results were clear: the 3D printer reduced production costs by 20–35% compared to manual compounding methods, cut total preparation time by approximately 10%, and reduced manual labour by 55%. It also dramatically decreased pharmacist exposure to API particles, a significant occupational health benefit for staff regularly preparing potent or sensitising compounds. Standard operating procedures validated during the study confirmed full compliance with Spanish and European pharmaceutical compounding regulations, establishing a practical, regulatorily defensible pathway for routine implementation.
In hospital pharmacy settings, where the pressure to prepare accurate doses for individual patients is acute and the consequences of dosing error are severe, automated gravimetric filling with 100% unit-level verification offers both a safety and an efficiency advantage. The compact footprint of a 3D printing unit means it can be installed within existing pharmacy infrastructure, and its electronic batch records support the traceability expectations of hospital pharmacy quality systems. Stability data generated on 3D printed formulations have demonstrated shelf lives of at least three months under standard storage conditions, sufficient for compounding applications where batches are typically prepared in response to near-term patient need rather than stockpiled. The on-demand production model provided by pharmaceutical 3D printing aligns naturally with traditions of pharmacy compounding practice.
References
1. FDA approves the first 3D printed drug product: Aprecia Pharmaceuticals [press release]. 2015.
2. Garba-Mohammed K., Bendicho-Lavilla C., Worsley A., Bonelli A., Haggan G., Hughes C., et al. 3D printing of dose-flexible crystalline solid dispersion tablets suitable for preclinical and first-in-human studies. Journal of Pharmaceutical Sciences. 2025;114(10):103943.
3. Bernhardt M.B., Shokraneh F., Hrizanovska L., Lahtinen J., Brasher C.A., Sandler N. Automated 3D printing-based non-sterile compounding technology for pediatric corticosteroid dosage forms in a health system pharmacy setting. Pharmaceutics. 2025;17(6).
4. Jin M., Zuo X., Blattner S.M., Frankenreiter S., Metzger M., Lu J., et al. 3D printing via melt extrusion deposition facilitates the use of extended-release profiles in preclinical research and development. Molecular Pharmaceutics. 2025;22(9):5428-42.
5. Seoane-Viaño I., Januskaite P., Alvarez-Lorenzo C., Basit A.W., Goyanes A. Semi-solid extrusion 3D printing in drug delivery and biomedicine: Personalised solutions for healthcare challenges. Journal of Controlled Release. 2021;332:367-89.
6. Denis L., Jørgensen A.K., Do B., Vaz-Luis I., Pistilli B., Rieutord A., et al. Developing an innovative 3D printing platform for production of personalised medicines in a hospital for the OPERA clinical trial. International Journal of Pharmaceutics. 2024;661:124306.
7. Rodríguez-Maciñeiras X., Bendicho-Lavilla C., Rial C., Garba-Mohammed K., Worsley A., Díaz-Torres E., et al. Advancing medication compounding: Use of a pharmaceutical 3D printer to auto-fill minoxidil capsules for dispensing to patients in a community pharmacy. International Journal of Pharmaceutics. 2025;671:125251.











