Artificial intelligence (AI) has evolved from a speculative concept to a cornerstone of Europe’s pharmaceutical industry, driving breakthroughs in drug discovery, clinical trial optimization, and patient care. Over the past decade, AI tools have slashed development timelines, enhanced precision in therapeutic targeting, and redefined interactions between healthcare providers (HCPs) and patients. Concurrently, regulators like the European Medicines Agency (EMA) and the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) are crafting frameworks to ensure AI’s ethical and safe integration. This article examines AI’s transformative role in pharma, the evolving regulatory landscape, and unresolved ethical challenges shaping the sector’s future.

Accelerating Drug Discovery through AI-Driven Innovation
Target Identification and Validation
Traditional drug discovery often requires years to identify viable disease targets, but AI proteomic, and clinical datasets to pinpoint proteins or genetic markers linked to diseases. For instance, Exscientia, an Oxford-based firm, reduced the timeline for identifying an obsessive-compulsive disorder treatment target from five years to 12 months by training models on chemical structures and biological interaction data1. This approach minimizes late-stage failures by prioritizing molecules with high binding affinity early in development.
Healx, a Cambridge startup, applies similar methods to rare diseases. Its AI platform aggregates patient records, preclinical data, and scientific literature to identify drug repurposing opportunities. In one breakthrough, Healx discovered that a Parkinson’s medication could treat Fragile X syndrome, advancing it to clinical trials within 18 months. These innovations highlight AI’s potential to democratize drug development for conditions traditionally neglected due to data scarcity.
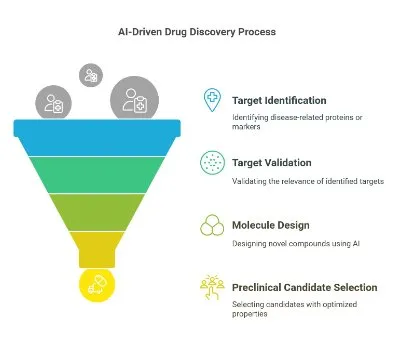
Generative AI in Molecule Design
Generative AI models, such as transformer-based architectures, now design novel compounds with optimized properties. These systems generate millions of virtual molecules, filtering them for solubility, toxicity, and target specificity. Bayer’s collaboration with Exscientia produced a preclinical oncology candidate with 10-fold greater selectivity than conventional methods. However, AI-designed molecules often overlook metabolic pathways or off-target effects, necessitating iterative lab validation.
Intellectual property (IP) complexities further complicate adoption. While the EU AI Act remains silent on AI-generated inventions, the European Patent Office mandates human inventorship for patents—a policy that risks stifling fully autonomous AI innovations. Balancing IP frameworks with ethical guardrails will be critical as generative tools advance.
Optimizing Clinical Trials through Intelligent Automation
Patient Recruitment and Stratification
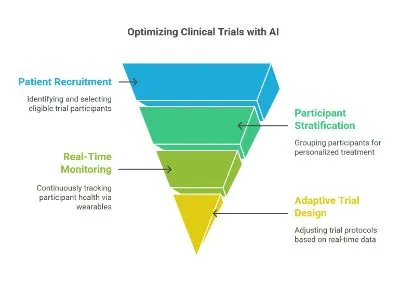
Nearly 80% of clinical trials face delays due to recruitment challenges. AI platforms like IQVIA’s Connected Intelligence analyze electronic health records, genetic data, and social determinants of health to identify eligible patients. In a recent oncology trial, natural language processing (NLP) parsed unstructured clinician notes to cut recruitment time by 40%. Predictive analytics further stratify participants into subgroups, enabling personalized dosing and clearer endpoints.
However, biased training data risk exacerbating health disparities. Algorithms trained on predo Sanofi Minantly European genomic datasets may underperform for African or Asian populations, skewing trial outcomes. The MHRA’s 2024 AI strategy addresses this by advocating “representative data governance,” including synthetic data generation to correct imbalances.
Real-Time Monitoring and Adaptive Trials
Wearables and AI analytics enable continuous remote monitoring, reducing site visits and improving retention. In a Novartis heart failure trial, smartwatch sensors detected early decompensation signs, triggering interventions that reduced hospitalizations by 25%. Adaptive trial designs, powered by reinforcement learning, dynamically adjust protocols based on interim results. Roche used this approach in an Alzheimer’s study to shift resources from amyloid-beta to tau protein inhibitors after preliminary data favored the latter.
Regulators are adapting: the EMA’s 2024 reflection paper endorses AI for “risk-based monitoring” but it requires rigorous validation to prevent false safety conclusions.
Enhancing Patient and HCP Engagement
Personalized Medicine and Adherence
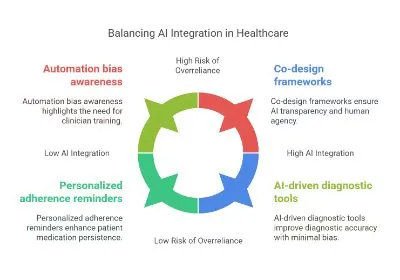
AI bridges population-level research and individualized care. BenevolentAI’s platform matches therapies to genetic profiles, improving response rates in heterogeneous conditions like lupus. For chronic diseases, AI apps deliver personalized adherence reminders based on behavioral patterns. A Sanofi-sponsored study found diabetic patients using such tools showed 30% higher medication persistence rate over six months.
Overreliance on algorithms, however, risks eroding clinician judgment. The European Patients’ Forum (EPF) advocates “co-design” frameworks, where patients and HCPs collaborate on AI development to ensure transparency and preserve human agency.
HCP Decision Support Systems
AI augments diagnostic accuracy across Europe. Siemens Healthineers’ AI-Rad Companion reduced missed tumor diagnoses by 18% in a UK pilot by flagging subtle imaging anomalies. Similarly, Babylon Health’s NLP tools parse clinical guidelines to generate context-aware treatment suggestions during consultations. The MHRA warns against “automation bias,” where clinicians uncritically accept AI outputs, emphasizing ongoing training and explainability protocols.
Regulatory Responses: Balancing Innovation and Safety
EMA and MHRA Strategies
The EMA’s 2024 workplan categorizes AI applications into three risk tiers:
• Low-risk: Predictive analytics for manufacturing (e.g., yield optimization).
• Medium-risk: AI-based clinical trial endpoints (e.g., imaging analysis).
• High-risk: Autonomous dose-adjustment algorithms.
High-risk applications require validation through “AI assurance labs,” auditing training data and model drift. The MHRA’s parallel strategy prioritizes interoperability with the UK’s Digital Health Technology Assessment framework, aligning with the EU AI Act’s sector-specific mandates.
The EU AI Act’s Implications
Enforced since August 2024, the EU AI Act imposes transparency requirements for high-risk medical AI, including detailed logs of training data and post-market performance. Research-phase AI is exempt from conformity assessments—a concession lobbied by the European Federation of Pharmaceutical Industries and Associations (EFPIA) to avoid stifling innovation. Nevertheless, compliance costs burden smaller biotechs, prompting calls for regulatory sandboxes.
Ethical Complexities in AI Deployment
Data Privacy and Consent
AI’s data demands clash with Europe’s General Data Protection Regulation (GDPR). Federated learning, where models train on decentralized datasets without transferring raw data, offers a compromise. AstraZeneca and Owkin used this method to develop a pan-European oncology model while preserving patient anonymity. However, GDPR’s “right to explanation” complicates opaque deep learning systems, necessitating advances in interpretability techniques.
Algorithmic Bias and Health Equity
Biased training data perpetuates disparities. An AI sepsis predictor underdiagnosed non-white patients due to imbalanced ICU records. The EPF recommends diversity quotas in trial datasets and independent bias audits, while the EMA promotes synthetic minority oversampling to correct imbalances without compromising privacy.
Transparency and Trust
A 2024 EPF survey found 68% of patients distrust AI tools lacking plain-language explanations. Explainable AI (XAI) methods like SHAP values are now regulatory prerequisites, despite added computational costs. Balancing transparency with performance remains pivotal for public trust.
Conclusion: Navigating the Future of AI in Pharma
Europe’s pharmaceutical sector stands at an AI crossroads, where innovation potential intersects with ethical imperatives. Companies like Exscientia and Healx demonstrate AI’s capacity to compress drug development timelines, while regulators race to update frameworks without stifling progress. Persistent challenges—data bias, IP ambiguities, and equitable access—demand multilateral solutions.
The EMA and the MHRA’s risk-based approaches provide a blueprint, but global alignment remains fragmented. Initiatives like the OECD’s AI Principles and ICH’s forthcoming pharmacovigilance guidelines could harmonize standards, easing compliance for multinational firms. Concurrently, patient advocates must co-design AI tools to ensure real-world relevance.
As generative AI advances, existential questions loom: Should AI-invented therapies be patentable? Can clinicians retain oversight in an era of autonomous diagnostics? Addressing these through inclusive dialogue will determine whether Europe harnesses AI to democratize medicine while upholding its ethical commitments.
References
1. EFPIA Position on AI in Medicinal Product Lifecycle
2. AI Drug Discovery in Europe
3. MHRA’s AI Regulation Strategy
4. AI in Clinical Trial Workflows
5. Challenges in AI Pharma Innovation
6. EPF Report on AI in Healthcare
7. Ethical Implications of the EU AI Act
8. EMA AI Workplan
9. AI in Clinical Trials (UK/EU)